
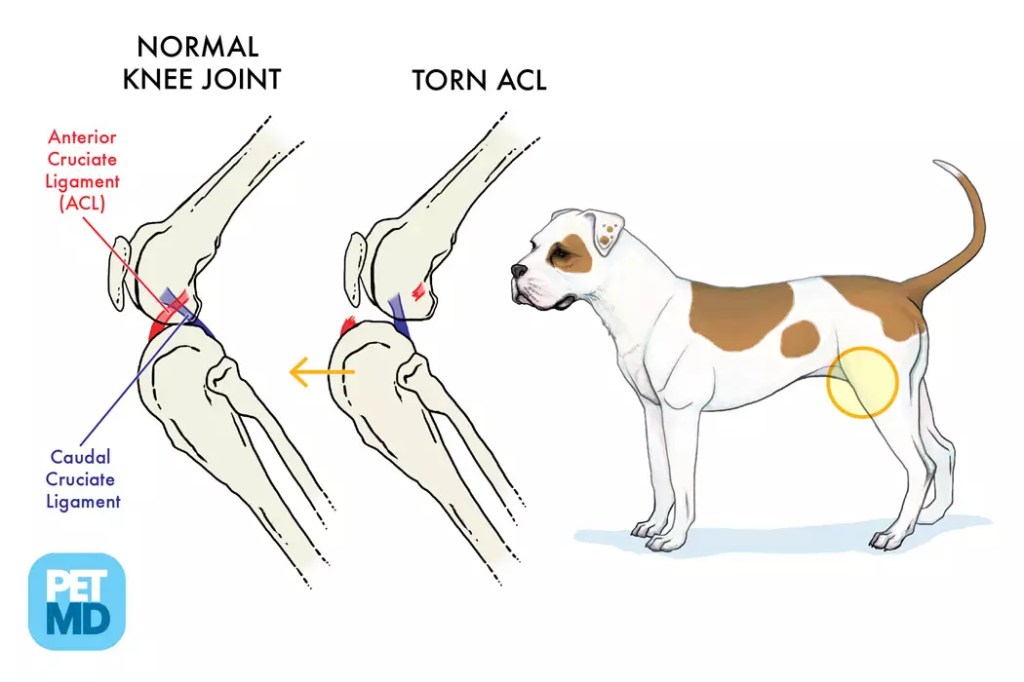
Cranial Cruciate Ligament (CCL) disease is the most common, painful knee injury in dogs and occasionally occurs in cats, and is caused by the rupture of a key ligament stabilizing the knee joint (stifle). Symptoms include sudden hind-leg lameness, limping, and joint swelling. It is often caused by degeneration, obesity, or injury during activity. Surgery is usually required to decrease joint damage and pain, as well as to assure joint function. The result of untreated CCL rupture is OsteoArthritis (OA). Although owners may try an orthotic support apparatus, those OFTEN do not offer adequate support unless manufactured for a specific patient. They are costly and inconvenient to use. Most dogs do best with surgical intervention. Cats however may do okay with rest and anti inflammatory treatment.
There are a variety of surgical options.****
Dogs weighing less than 40-50# may do okay with a less aggressive/complicated/expensive surgical procedures:
- Lateral Suture (Extracapsular) Repair and the TightRope technique. These methods are often preferred for small-to-medium dogs as they stabilize the knee from the outside using prosthetic material rather than cutting bone. However, larger dogs, especially those weighing over 60#, have better long-term outcomes with more complicated surgical procedures, ideally performed by surgical specialists who perform dozens of these procedures yearly, versus a general practitioner who may do less than 2-3 of these surgeries yearly. Patients who have physical therapy after surgery usually do remarkably well.
According to published data the most successful surgical procedures for dogs weighing over 60# are TPLO (Tibial Plateau Leveling Osteotomy) or TTA (Tibial Tuberosity Advancement) procedures.
****Surgical Procedures available:
For dogs weighing less than 40-50#:
- Extracapsular repair/Lateral Suture Technique: One of the oldest of the CCL repairs. In simplest terms, a suture material (artificial cruciate ligament) is placed from the back of the knee joint around to the front of the knee, acting like an artificial CCL. One small bone tunnel is necessary to perform this procedure. The suture material tends to stretch or break prior to strong enough fibrosis to occur to help stabilize the knee.
Or,
- Tightrope Technique: The Tightrope technique, which is the latest procedure for smaller dogs, was designed to be a minimally invasive procedure that augments the principles of the lateral suture technique by increasing stabilization from bone to bone fixation at highly researched isometric points on both the femoral and tibial sides of the limb. Newer and improved stronger implants that were developed for this technique will allow for stronger stabilization of the knee. This stronger and improved material stabilizes the knee to allow for improved periarticular fibrosis in the post-operative recovery phase, allowing the patient to get back to a more normal life prior to the ligament rupture.
For dogs weighing over 60#:
- TTA (Tibial Tuberosity Advancement): This is a surgical procedure which involves cutting the top of the tibia and moving it forward and stabilizing it in a new position with implants.
And,
- TPLO (Tibial Plateau Leveling Osteotomy): The TPLO is considered the gold star standard in cruciate rupture. It is also considered the most invasive and most expensive procedure due to the complexity and specialized plating and screw systems applied to the repaired limb. The way this procedure works is by eliminating what is called the Cranial Tibial Thrust, which are the forces that cause the damage to the cranial cruciate ligament in the first place. This procedure is considered the best form of stabilization of the Cruciate Deficient Stifle. Although not every procedure is right for all pets, this procedure is best for most.
The difference between TPLO and TTA is not that easy to explain simply.
TPLO cuts the tibia and changes the alignment of the top of the tibia relative to the forces that are applied so that the stifle becomes stable without an intact CrCL.
TTA also involves cutting the tibia, then moving the attachment of the quadriceps tendon (which applies one of the main forces to the stifle) relative to the tibial plateau.
So both involve a tibial osteotomy that is stabilised with a bone plate and in general we say that TPLO moves the bone to meet the force, and TTA moves the force to meet the bone. The effect of both is to neutralise the forces acting on the knee to cause a cranial displacement of the tibia with respect to the femur during weight bearing.
Both procedures have standard and unique sets of complications. In general though, at this stage, the complication rate for both is relatively low provided that the surgeon is experienced in the technique.
Both techniques effectively neutralise instability in the knee during weight bearing. By Dr. Kathy S ©Copyrights 2026

You must be logged in to post a comment.